Musculoskeletal PRP Applications
Harnessing the Regenerative Potential of PRP in MSK Medicine
Platelet-Rich Plasma (PRP) is an effective regenerative therapy in orthopaedic and sports medicine, supporting tissue healing in tendons, ligaments, cartilage, and muscle. By delivering a concentrated dose of autologous growth factors and bioactive proteins directly to the site of injury, PRP offers a minimally invasive alternative to surgery or corticosteroids for a wide range of musculoskeletal conditions.
Alocuro’s PRO-PRP system delivers consistently high platelet concentrations with control over leukocyte inclusion, enabling clinicians to tailor the PRP formulation to the specific needs of the tissue being treated.

How PRP Supports Tissue Healing
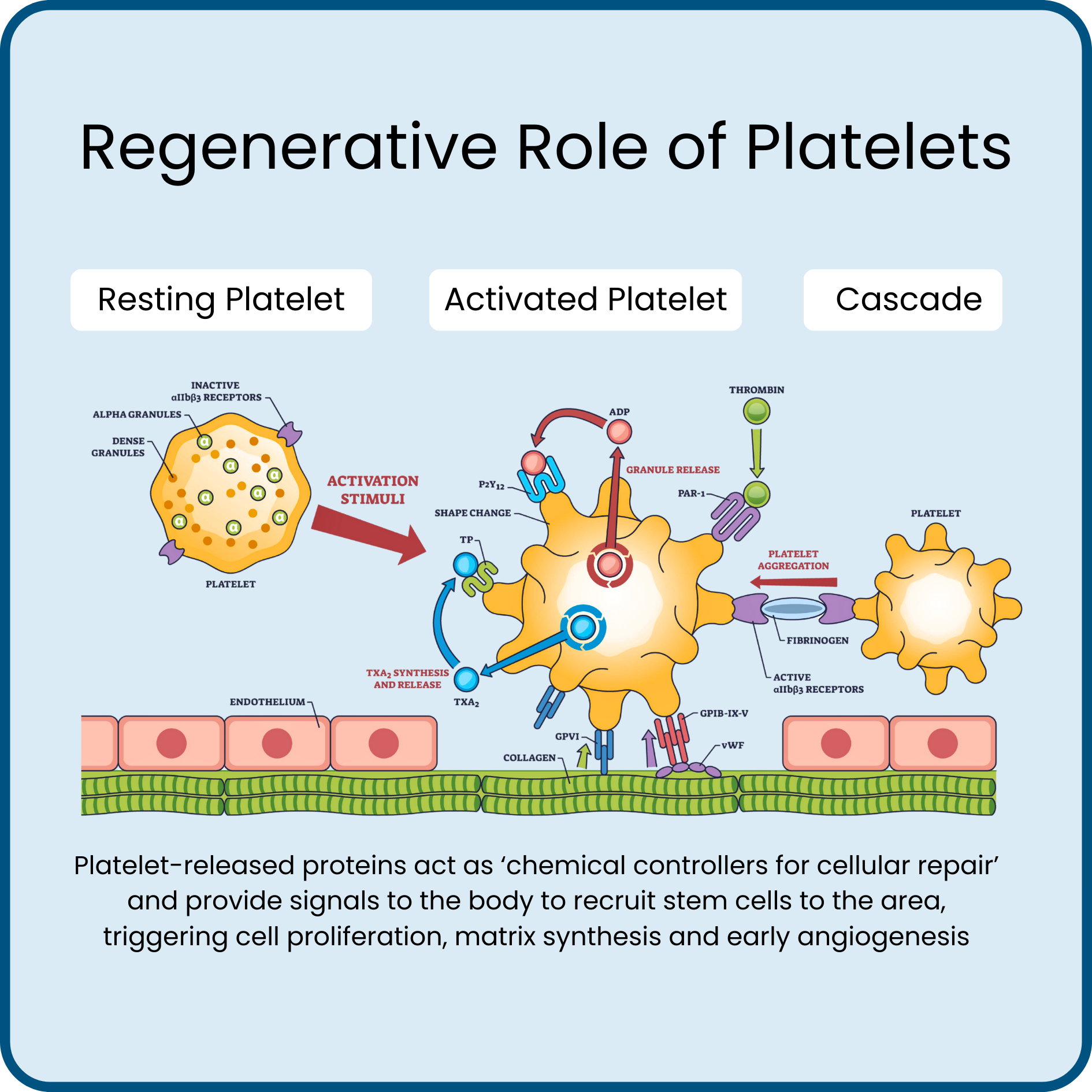
Upon activation, platelets release a complex mixture of growth factors, cytokines, and signalling molecules from their α-granules and dense granules.
These bioactive proteins work as ‘chemical controllers’ and play a key role in:
Modulating the inflammatory response
Recruiting reparative cells
Stimulating angiogenesis
Promoting collagen synthesis and extracellular matrix remodelling
This effects are particularly useful in avascular tissues (e.g. tendons, cartilage), where natural healing is limited due to limited blood supply.


Clinical Indications for MSK PRP
PRP is typically used as part of a multidisciplinary approach to treating the patient symptoms while encouraging healing and regeneration of the injured or degenerative tendon, joint, muscle or ligament.
In elite athletes it is commonly used to reduce the time needed for recovery from injury, and to provide a more elastic healing tissue interface, and may reduce the risk of retear in the case of tendon injuries.
Tendinopathies
Lateral epicondylitis (tennis elbow)
Patellar tendinopathy
Achilles tendinopathy
Rotator cuff tendinopathy
*PRP has shown to outperform corticosteroid injections in long-term pain and function outcomes in many Level 1 clinical trials.
Ligament Injuries
Partial tears
Mild to moderate ankle strains
Osteoarthritis (Intra-Articular Use)
Knee OA (Kellgren-Lawrence grades I–III)
Hip OA (early stage)
Glenohumeral and Acromioclavicular joint OA
*PRP has demonstrated pain and function improvement beyond hyaluronic acid or placebo in multiple RCTs, particularly at 6–12 months follow-up.
Muscle Injuries
Grade II hamstring, adductor, or quadriceps strains
Recurrent muscle tears
*PRP may reduce re-injury risk and time to return to play when used alongside rehabilitation.
Post-Surgical Applications
Meniscal repair
ACL reconstruction
Tendon repairs
*Used intra-operatively to enhance healing response and reduce scar tissue formation.

Alocuro Precision for Musculoskeletal PRP
Alocuro’s PRO-PRP system is engineered to meet the specific demands of musculoskeletal and orthopaedic PRP applications:
Platelet concentration up to 12× baseline is possible, optimised for dense connective tissue and cartilage environments. Typically 3-6X is used.
90% platelet recovery efficiency average, delivering evidence-aligned doses.
Customisable leukocyte profile, allowing production of leukocyte-rich PRP and leukocyte-poor PRP for intra-articular or cartilage applications.
No thixotropic gel or artificial separator medium, avoiding unwanted chemical residues and nil risk of accidental aspiration of gel within PRP injectate.
ARTG-listed, sterile, closed-system for procedural safety and compliance.
Ideal Patient Profile
PRP is most effective when applied to:
Localised pathology confirmed by clinical and/or imaging findings
Mild to moderate degenerative changes (OA)
Partial tears and non-retracted injuries
Cases that have failed first-line conservative treatment (physio, NSAIDs)
Patients who have healthy lifestyle
Not suitable for systemic inflammatory arthritis, active infection, or malignancy.
Treatment Protocol & Expectations
Injection typically performed under ultrasound guidance for accuracy.
Post-injection response: Mild inflammatory flare (24–48 hours), followed by gradual symptom improvement.
Patients may require 1–2 treatments, typically spaced 4 weeks apart.
Best outcomes when combined with graded rehabilitation, biomechanical correction, and load management.
Evidence-Based Outcomes
In randomised-controlled trials, PRP has demonstrated:
Superior long-term outcomes to corticosteroids for tennis elbow & patellar tendinopathy.
Delayed OA progression and reduced pain scores in early-to-moderate knee osteoarthritis.
Improved tendon structural healing on ultrasound or MRI post-treatment.